Urgent Care 1 Group

Serving The Metropolitan Detroit Area

By S.Nasry, M.D. Volume 3
Pneumonia is the 7th leading cause of mortality in the US causing over 900,000 deaths annually especially in patients older than 65. Risk factors include smoking, COPD and Alcoholism.
Pneumonia can be caused by Bacteria, Viruses or fungi. recent studies gave conflicting results, one study showed that viruses are more common than Bacteria while the other study showed the opposite.
The lung tissue is normally sterile or has no bacteria and lung infection or pneumonia occurs usually when the bacteria and other pathogens that reside in the non-sterile mouth and throat descend to the lung tissue and trigger intense inflammatory reaction that causes the classic symptoms of pneumonia: Fever, purulent cough, shortness of breath and chest pain (from irritating the lung cover known as the Pleura that is quite rich with pain receptors nerve endings in contrast to the lung tissue that has none).
A strong cough reflex is our main defense mechanism against these descending microbial invaders and all conditions that can weaken cough will increase the risk of developing Pneumonia such as old age, muscular fatigue, malnutrition and altered mental status (nursing home patients).
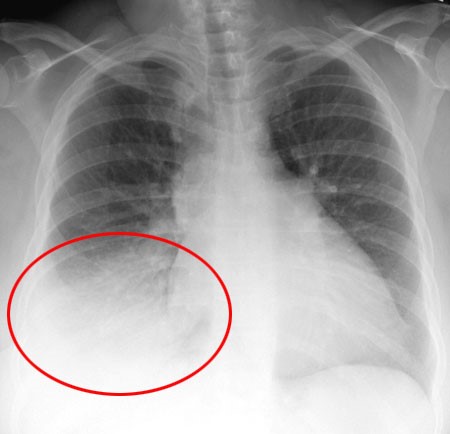
Pneumonia is usually diagnosed by exam and lungs auscultation (50% sensitivity) or by chest X-Rays (near 100% sensitivity) that is why a chest X-Rays is recommended whenever Pneumonia is suspected.

Medical Director
S. Nasry, M.D.
Determining the exact bacteria or virus causing Pneumonia was limited in the past to ICU patients but now with the emergence of PCR testing we can test patient's sputum for a long list of common pathogens to determine the exact cause quite rapidly however this test is expensive and unwarranted at this time since empiric treatment (treatment that targets the common pathogens) is effective.
When diagnosing Pneumonia, the doctor has to determine if the patient may be treated safely with oral antibiotics at home or he should be referred for in hospital IV antibiotics. The age, the vital signs, the hydration status and the presence of chronic debilitating diseases all play a role in the decision making.
In our urgent care we can offer you a physical exam, a chest X-Rays, antibiotic injections, establish the Pneumonia diagnosis,start the proper treatment and refer when necessary to the hospital.
By S.Nasry, M.D. Volume 2
Pain is a dreadful and hated symptom that can disturb people's life and paralyze their daily routines, stop them from working or reduce their productivity and sometime destroy careers and ruin future.
Pain is a manifestation of a body derangement that our creator gave us as an alarm so we can seek a cure and not to be tortured, the great majority of pain causes are curable or treatable from heart attacks to broken bones, almost all with proper treatment -except for the terminally ill cancer patient and rare other illnesses- pain quickly abates with proper treatment.
It has been our practice to provide pain medications with some liberty to those visiting our clinics with acute illness or trauma as long as we can verify a disease process that causes pain. It is my belief as a physician that it is my duty to combat pain whenever there is an honest patient with legitimate cause of pain.
Over the last 5-10 years a new problem has emerged or become more significant, it is the Narcotics dependence and addiction. while physicians were trying to wipe out pain narcotics started causing especially when used or abused for extended period of time-started causing a new catastrophic problem, instead of curing pain and putting people back on the normal life and productive work track we derailed their destiny to a miserable life of incapacity and drug seeking behavior. what went wrong? Many factors played a role including the loose surveillance, the blind doctor patient trust and patients selling their medications and sometimes using it more frequently and for longer period than medically recommended just like street drugs!!!
Medical Director
S. Nasry, M.D.
The CDC (Center for disease control) took the initiative in March of 2016 and published guidelines for physicians to follow aimed at reversing the Narcotics dependence epidemic, the net result was much less pain pills recommended for acute pain and much stricter surveillance and tougher rules for chronic pain management. In addition, we now use routinely MAPS system (Michigan Automated Prescription System). It allows us to see all controlled meds prescribed by different physicians for one patient on line So when people are coming to our clinics for chronic pain evaluation we can quickly tell if they have been "Narcotics shopping" seeking meds from multiple prescriber's or using different pharmacies.
Our dear patients just like the stricter new rules for antibiotics prescriptions (please see the June newsletter) we are now entering a new era of pain management and you should expect less pain pills probably enough for 3-5 days only (CDC Rule) simply because now we have DUAL RESPONSIBILITY:
By S.Nasry, M.D. Volume 1
With the rapid spread and implementation of electronic health record (EHR) the government and its health organizations are getting more and more involved in monitoring doctors adherence to practice guidelines and their deviation from it in some circumstances penalizing those who are not compliant.
With the emergence of resistant bacteria that are baffling scientists, it is quite prudent to increase the pressure on doctors to slow down the crazy old practice that an antibiotic is cure for all infections!!! Did you know that US consumption of antibiotics is about 50% of the world consumption!!
Hence, doctors nowadays are having tinnitus from something called "Antibiotic Stewardship". Every conference we attend we hear repeatedly this outcry for sensible, intelligent, and accurate antibiotic use, and get threatened in bold terms if we do not comply with financial sanctions and payments cuts!!! Most of us by now are on board with this rally and have implemented stricter rules and we are posting in our clinics (Urgent Care 1 Group) posters that will help doctors explaining to the Z-PAK addicted customers when it is proper to give an antibiotic.
Most of the problem however is not the doctors bad habit but rather deep public conviction in this deep seated false perception. We are facing mixed responses when we decline prescribing antibiotics, on one hand the intelligent patients usually appreciate and thank us for explaining why the antibiotic is not necessary and on the other hand we sometimes are faced with the not so smart patients who are convinced that the antibiotic is the cure no matter what the cause is.
Medical Director
S. Nasry, M.D.
One day I was working in our Garden City Office, a woman and her teenage son walked in, he has cold symptoms for 2-3 days, after taking history and doing physical exam it was quite clear that the son has a cold, I tried to explain to the mother why this is a cold, she interrupted me with some rudeness and asked: "Are you going to give him a Z-PAK?" I replied no, she stormed out of the room telling her son: "Let's go to another clinic". We care tremendously about our patients but part of this care is to give an accurate diagnosis and to prescribe the right medicine while adhering to the national practice guidelines. Our dear patients need to understand that the old Z-PAK JUST ASK days are over and they should be happy because this means better medicine practice now and less resistant bacteria in the future.
Sign up for our newsletter and keep up to date:












